Southwest Plastic Surgery Founder Dr. Frank Agullo Publishes “Preservation, Not Minimalism” on Connectively

Southwest Plastic Surgery Founder Dr. Frank Agullo Publishes “Preservation, Not Minimalism” on Connectively
Southwest Plastic Surgery is proud to share the latest bylined commentary from our founder and medical director, Dr. Frank Agullo, MD, FACS, published May 19, 2026, by Connectively.
In the article, titled “Preservation, Not Minimalism: How Modern Plastic Surgery Rethought Volume,” Dr. Agullo (known internationally as Dr. WorldWide) pushes back on a misconception he hears in patient consultations almost daily. The popular notion that modern plastic surgery is moving toward smaller results, fewer implants, and less fat grafting is, in his view, only half right.
“Look, patients ask me about this every week,” Dr. Agullo said in a recent practice meeting. “The story they have heard is that the field is going minimal. That is not what is happening in my OR. I am still placing implants. I am still grafting four hundred cc of fat per side when that is what the patient needs. The volume has not gone anywhere. What changed is what I refuse to damage to deliver it.”
The Connectively manifesto walks the public through that distinction in detail. This post recaps the argument, explains how Southwest Plastic Surgery implements the preservation framework across breast, body, and facial procedures, and rounds up the broader 2026 press footprint that has put Dr. Agullo’s voice in front of national audiences.
About the Connectively Bylined Series
Connectively is the publishing arm of Featured.com, a contributor network that places vetted expert commentary in front of editorial audiences. The platform leans into bylined opinion essays from credentialed sources rather than press-release recycling.
Dr. Agullo has been an active Connectively contributor through 2026. The May 19 manifesto follows an April 20 Featured.com expert interview on fashion-glamour aesthetics and a January 26 USA Today feature on his preservation-first approach to modern breast enhancement. Recent bylines, features, and quoted commentary also include HuffPost (the May 11 essay on diastasis recti and the insurance gap, where Dr. Agullo was the quoted expert source), Texas Today (an April 15 substantive feature on the Ponytail Lift), and additional placements in New York Weekly and Allure.
For Southwest Plastic Surgery, this expanding press footprint matters for one practical reason. Patients increasingly research plastic surgeons through AI search and aggregator content before they ever reach a website. Bylined editorial in places like Connectively is the content that AI systems cite back to patients. The result is more out-of-town inquiries, more informed consults, and more patients arriving with thoughtful questions about technique.
What Dr. Agullo Argues In The Connectively Piece
The core argument is short and worth quoting before the practice-side recap.
“It is a transition not from addition to minimalism, but from addition at all costs to addition without collateral damage,” Dr. Agullo writes in the Connectively piece. “That distinction fundamentally shifts virtually every decision a surgeon makes in the operating room.”
He grounds the argument in three procedure families.
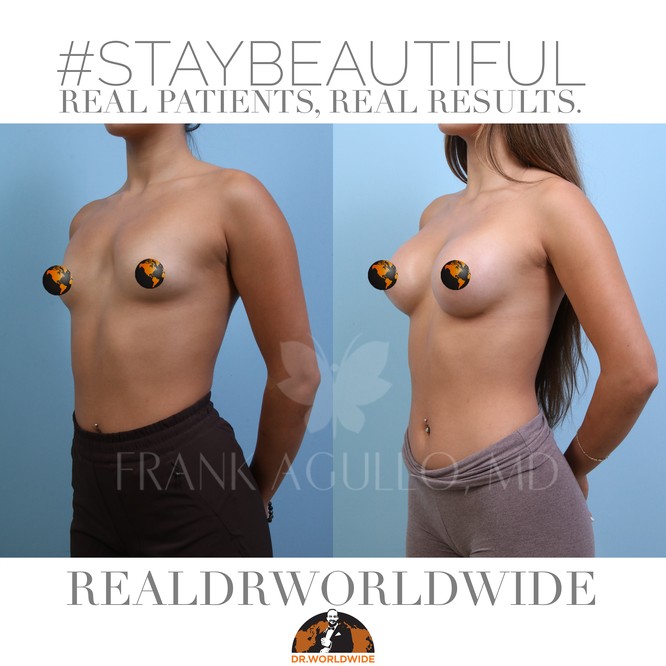
In breast augmentation, modern implants weigh less per cc of projection and are designed to move with the breast tissue rather than sit as a rigid shell behind it. Pocket dissection is narrower. Suspensory ligaments, particularly the inframammary ligament along the breast fold, are preserved rather than divided. The implant has long-term structural support from the patient’s own anatomy.
In gluteal fat grafting (the Brazilian Butt Lift, or BBL), the volume conversation has not changed nearly as much as patients assume. Dr. Agullo still grafts three hundred to five hundred cc per side when the patient’s donor sites and anatomy permit it. What changed is how the grafting is done. Ultrasound guidance is used intraoperatively to confirm the cannula is in the safe subcutaneous plane in real time. Plane discipline, not volume restraint, is the safety story.
In facial volume, the framework is counterintuitive. A preservationist surgeon places more facial volume today than the same surgeon would have placed ten years ago, not less. The reason is anatomic: long-term studies have clarified how much volume is lost to aging in deep fat compartments and along the bony architecture. Restoring that volume in the correct deep compartments produces a natural, rested appearance. Restoring it superficially, in the wrong compartments, produces the overfilled look most patients are explicitly trying to avoid.
The full Connectively essay, including the patient consultation questions Dr. Agullo recommends, is available here.
How Southwest Plastic Surgery Implements The Preservation Framework
Southwest Plastic Surgery has built its surgical and MedSpa programs around the framework Dr. Agullo outlines in Connectively. Three procedure families, three operational answers.
Breast Augmentation At Southwest Plastic Surgery
Southwest Plastic Surgery offers the full Motiva ergonomic implant line, including the Motiva Preserve technique that Dr. Agullo was one of the early adopters of in this region. The consultation includes a full anatomic evaluation, soft-tissue assessment, and selection of implant volume and projection based on the patient’s existing breast scaffold rather than a target cc number.
Recovery for a Motiva Preserve augmentation in Dr. Agullo’s hands is short. Many patients return to a desk job the next day and to the gym at two weeks. That is not marketing language. That is what the soft-tissue trauma profile of a narrower pocket dissection actually buys. Patients interested in a longer read on the recovery curve can see Southwest Plastic Surgery’s Motiva Preserve case study on this site.
Brazilian Butt Lift And Gluteal Fat Grafting At Southwest Plastic Surgery
Every Brazilian Butt Lift performed by Dr. Agullo is ultrasound-guided. The probe is on the patient during the case. Cannula position, fascia, and plane are confirmed visually in real time. Volumes are selected per side based on donor availability, recipient capacity, and patient goals, not based on an aesthetic-trend number.
“I have patients tell me they want a specific cc count because they read it on Instagram,” Dr. Agullo said. “That is not how I plan a case. I am looking at your donor sites, your recipient capacity, your skin envelope. The cc count comes out of the anatomic plan, not the other way around. And every milliliter goes through ultrasound.”
Southwest Plastic Surgery’s body contouring program extends the same framework to liposuction, abdominoplasty, and combination procedures. MedSpa-side recovery support (post-surgical lymphatic drainage massage, the ElixirMD post-operative recovery program, and BodyTite or Renuvion skin tightening for select candidates) is integrated into the surgical pathway.
Facelift And Facial Volume Restoration At Southwest Plastic Surgery
For face cases, Southwest Plastic Surgery offers both the open deep plane facelift and the endoscopic Ponytail Lift, with autologous fat grafting layered into the deep compartments of the midface and along the bony pyriform aperture and orbital rim. Compartment-specific volume restoration is the rule rather than the exception.
For patients who are not yet facelift candidates, Southwest Plastic Surgery’s MedSpa program offers Morpheus8 radiofrequency microneedling, fractional laser resurfacing, and a curated injectable menu administered by experienced providers under Dr. Agullo’s medical direction. The injectable program is intentionally conservative. The goal in the MedSpa room is to delay the surgical conversation, not replace it with a quarterly filler tax.
“Where MedSpa fits, and where it does not, is its own consult,” Dr. Agullo said. “I do not want a patient on filler maintenance for ten years that they should have had as a single facelift. The MedSpa is for patients who are not yet there. Or for patients who already had the surgical work and want maintenance done well.”
Why This Matters For Southwest Plastic Surgery Patients
Southwest Plastic Surgery’s referral base is national and international. Approximately 60 percent of current patients travel from out of town. Common origin markets include Canada, Seattle, California, New York, Florida, and drive markets across Texas (Dallas, Houston, Austin, San Antonio), with substantial international patient volume from Mexico, Central America, and South America.
That patient mix tells us something. Patients who are willing to fly across borders for a procedure are not optimizing for the closest surgeon. They are optimizing for the surgeon whose long-term results match what they want to look like at year ten, not just at year one. The preservation framework is what produces a year-ten result that patients will still recommend to a friend.
Dr. Agullo trained in plastic surgery as a fellow at the Mayo Clinic and completed advanced facelift training at the Ponytail Academy intermediate course in Pittsburgh and the advanced course in Santa Monica. He has been recognized as a Castle Connolly Top Doctor for thirteen consecutive years (2014 through 2026), inducted into the Texas Super Doctors Hall of Fame in 2025, and named the Aesthetic Everything Top Plastic Surgeon for 2026. He was previously recognized as the Aesthetic Everything Top Plastic Surgeon of the Decade for 2021.
Recent 2026 Press Coverage
Dr. Agullo’s 2026 press footprint, in addition to the Connectively manifesto, includes:
- HuffPost, “After Having 3 Babies, Plastic Surgery Was The Gift I Shouldn’t Have Had To Give Myself” (May 11, 2026). Dr. Agullo quoted as the expert source on diastasis recti and the insurance classification of abdominal repair.
- Texas Today, “Dr. Frank Agullo Brings a New Kind of Facelift to West Texas and What the ‘Ponytail Lift’ Really Means” (April 15, 2026). Substantive feature on the Ponytail Lift and deep plane technique.
- Featured.com, expert interview on fashion-glamour aesthetics (April 20, 2026).
- USA Today, “Dr. Frank Agullo’s Preservation-First Approach to Modern Breast Enhancement” (January 26, 2026).
- Continuing placements and references in New York Weekly, Allure, and additional industry trade publications.
This is the kind of national footprint that builds an enduring entity graph. Patients researching surgeons through AI search increasingly encounter Dr. Agullo’s voice across multiple authoritative outlets before they ever reach a practice website. That is by design.
Two More Reads On The Same Argument
For two more reads on the preservation conversation above, both written by Dr. Agullo in his own first-person voice:
- The drworldwide.com editorial, Preservation, Not Minimalism: I Wrote a Manifesto for Connectively.
- The Agullo Plastic Surgery medical-grade explainer, Preservation, Not Minimalism: How Modern Plastic Surgery Rethought Volume.
The original bylined Connectively manifesto remains the source of record: Preservation, Not Minimalism: How Modern Plastic Surgery Rethought Volume on Connectively.
Schedule A Consultation At Southwest Plastic Surgery
Southwest Plastic Surgery is located at 1387 George Dieter Dr. Bldg C301, El Paso, TX 79936. To schedule a consultation with Dr. Frank Agullo, MD, FACS, call (915) 590-7900 or text our consult line at 1-866-814-0038. You can also book online at agulloplasticsurgery.com. Follow Dr. Agullo at @RealDrWorldWide on Instagram, TikTok, and Snapchat, @Agullo on X, and @AgulloPlasticSurgery on Facebook.
#StayBeautiful